What is Thalassaemia?
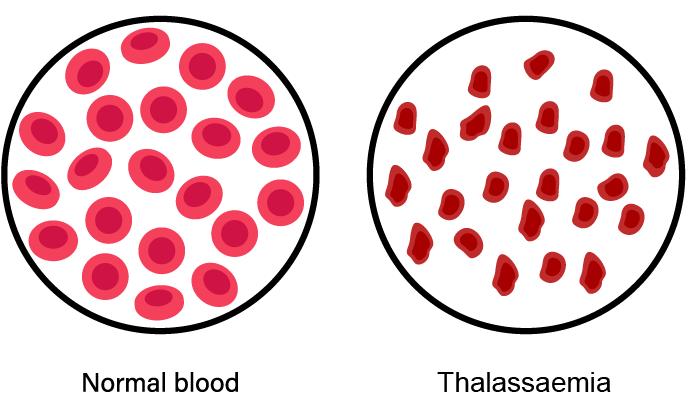
Thalassaemia is a genetic blood disorder that causes haemoglobin deficiency and severe anaemia, starving organs of oxygen, which inhibits their ability to function properly.
Once universally fatal, today Thalassaemia can be treated as a chronic disease. The major cause of illness and mortality has shifted from haemoglobin deficient anaemia to iron overload associated with chronic blood transfusion therapy. With medical advances, leading-edge technology, and scientific research, people with Thalassaemia are living longer.
Thalassaemia represents a group of genetic blood disorders with a wide variety of associated symptoms that commonly appear in the first two years of life.
Symptoms may include:
- Skin with pale, jaundiced or anaemic appearance
- Slow growth
- Poor appetite
- ‘Failure to thrive’
- Fatigues easily
- At risk for infections